
Advancing Non-Contact Vital Sign Monitoring: Heart Rate and Respiratory Rate Sensing with RF-PMD
1. INTRODUCTION
Non-contact physiological monitoring represents a significant unmet need across medical, defense, and consumer health settings. Existing vital sign monitoring modalities such as electrocardiography, pulse oximetry, and respiratory belts all require physical attachment to the patient, creating barriers to continuous monitoring where sensor adherence is impractical, infection control is a concern, or field conditions preclude wearable deployment.
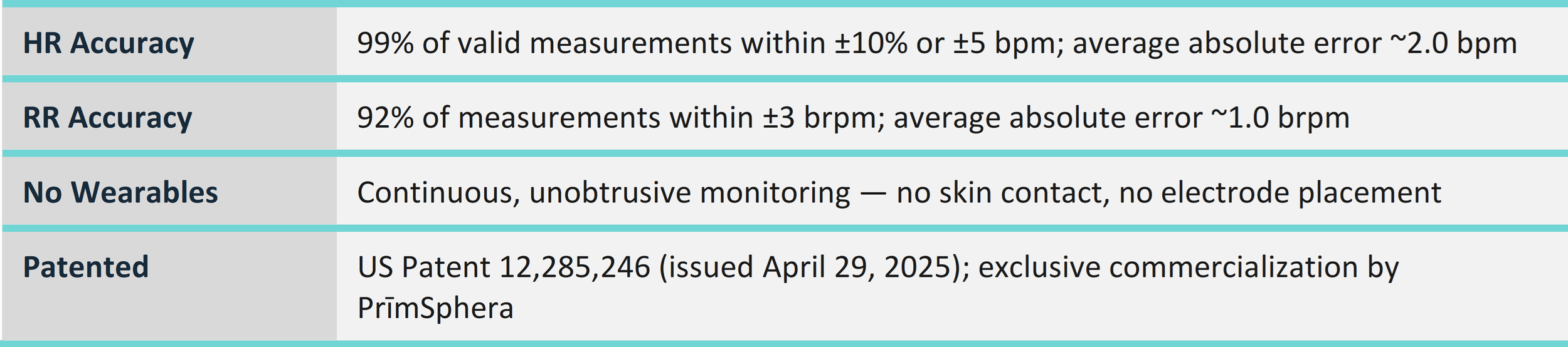
VitalSense, developed by PrīmSphera, Inc. in collaboration with the University of Notre Dame, addresses this gap through Radio Frequency (RF) signals alone. The system requires no wearable devices and no physical contact with the user. Each measurement or reading is taken passively from the users 's perspective.
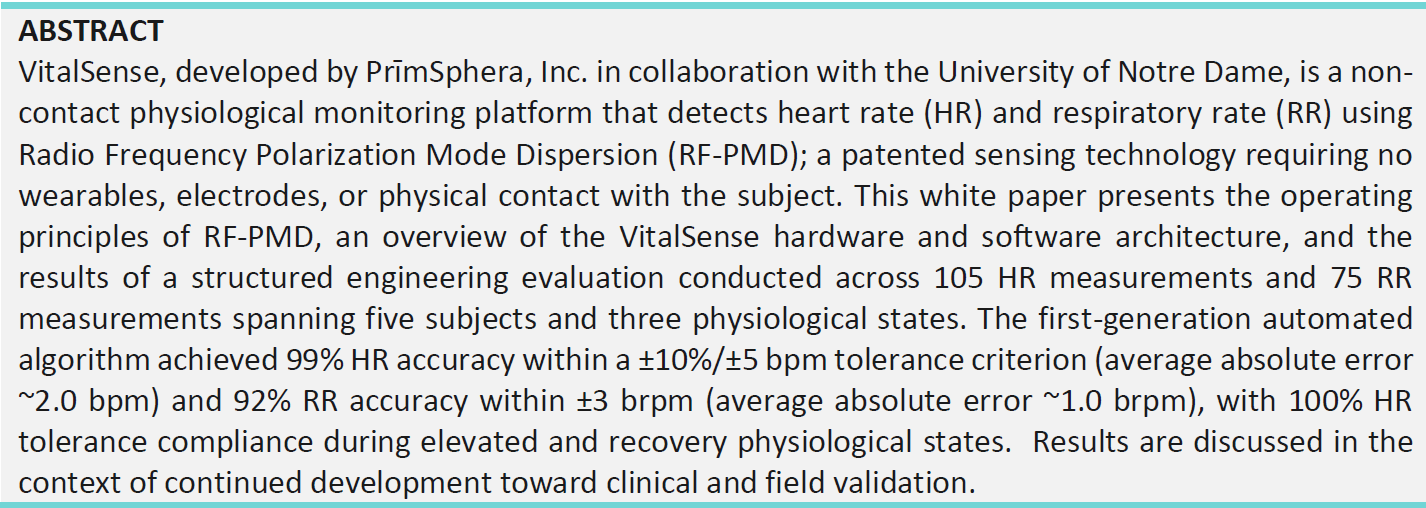
This paper presents the operating principles underlying RF-PMD, an overview of the VitalSense platform architecture, and the results of a structured engineering evaluation conducted in late 2025. Testing spanned 105 HR measurements and 75 RR measurements across five subjects and three physiological states, progressing from exploratory characterization through full algorithm integration in production demonstration software. As shown below, the first-generation automated algorithm achieved 99% HR accuracy within protocol tolerance and 92% RR accuracy within ±3 brpm, with an average absolute HR error of approximately 2.0 bpm.
2. THE PROBLEM: GAPS IN CONTINUOUS PHYSIOLOGICAL MONITORING
Continuous vital sign monitoring is critical across a wide range of settings such as intensive care, emergency response, long-duration field operations, and consumer health. Yet every mainstream monitoring modality requires physical attachment to the patient:
Electrocardiography (ECG) requires adhesive electrodes applied to bare skin.
Pulse oximetry requires a clip or probe on a finger, earlobe, or forehead.
Respiratory belts and capnography require chest straps or nasal cannulas.
Wrist-worn wearables are subject to motion artifact and patient compliance issues.
These constraints create real-world barriers: skin irritation and electrode failure in long-duration monitoring, infection-control concerns in multi-patient clinical environments, difficulty of deployment in neonatal or trauma contexts, and impracticality in austere field settings. The following section describes how RF-PMD addresses each of these constraints.
3. TECHNOLOGY BACKGROUND: RF-PMD
The VitalSense platform is built on RF Polarization Mode Dispersion (RF-PMD), a patented sensing technology invented at the University of Notre Dame by Dr. Thomas Pratt and exclusively licensed to PrīmSphera, Inc. The RF-PMD technology leverages a fundamental but underexploited property of radio wave propagation.
3.1 Exploiting Multipath as a Sensor
When an RF signal travels from transmitter to receiver, it rarely follows a single direct path. Instead, it reflects off walls, furniture, and the human body which generates a rich ensemble of propagation pathways; also referred to as multipath. Traditional wireless systems treat multipath as interference to be suppressed. RF-PMD does the opposite: it deliberately exploits multipath as a carrier of environmental information.
Because RF signals can penetrate many materials (wood, glass, and to varying depths, biological tissue) while being blocked by others (metal), the multipath structure of a room is exquisitely sensitive to physical changes; specifically, the millimeter-scale chest-wall displacement produced by each breath or heartbeat.
3.2 Polarization Mode Dispersion and the Poincaré Sphere
RF-PMD captures these changes via the polarization state of the received signal. Polarization is defined by the relative amplitudes and phases at two orthogonal receive antennas. Any shift in the propagation environment produces a corresponding shift in polarization state.
Polarization state is represented mathematically by four Stokes parameters and visualized as a point on the Poincaré sphere. When a wideband signal is transmitted, different frequency sub-bands undergo different polarization shifts as they propagate through the channel. This frequency-dependent spreading of polarization states across the sphere is Polarization Mode Dispersion (PMD), and the resulting curve is the PMD signature; a unique fingerprint of the transmitter–channel–receiver path.
3.3 Sensing Advantages Over Conventional RF Techniques
The PMD signature offers two critical advantages for physiological sensing:
Frequency-domain signal-to-noise ratio (SNR) integration: Rather than integrating signal energy only across time, RF-PMD integrates across the signal bandwidth. This improves SNR without sacrificing temporal resolution which is essential for capturing fast physiological signals such as heart rate.
High-sensitivity change detection: Any physical change that alters the multipath structure, such as the subtle mechanical activity of the heart, produces a measurable change in the PMD signature. This enables non-contact detection of physiological signals that would be invisible to single-frequency or narrowband RF systems.
3.4 Coherent Signal Dispersion (CSD) and MIMO Extension
PrīmSphera extends the RF-PMD framework to Coherent Signal Dispersion (CSD), incorporating spatial diversity through multi-input, multi-output (MIMO) antenna configurations. Space-domain CSD measurements are combined with frequency-domain PMD data in a coherent sensing matrix, significantly improving robustness across subjects, environments, and physiological conditions.
3.5 Patent Protection
The foundational RF-PMD and CSD technologies are covered by patents exclusively licensed to PrīmSphera. The specific application of RF-PMD to heart rate and respiratory rate sensing is additionally protected by US Patent 12,285,246, issued April 29, 2025.
4. THE VITALSENSE SYSTEM
The tangible components of the VitalSense platform are a proprietary software defined radio (SDR), an optimized antenna array, and a web-based graphical user interface (GUI) or a software client application depending on the actual deployment model.
4.1 The VitalSense Hardware
The VitalSense device is a free-standing sensor integrating a software-defined radio (SDR) built on AMD's RF-SoC platform, a multi-element, dipole 2.4 GHz antenna array optimized for RF-PMD, and embedded algorithm execution. No component is attached to or worn by the subject. The system communicates via TCP/IP with a host PC client that provides a live GUI, real-time HR and RR plotting, and CSV data export.
4.2 The VitalSense Software
The HR/RR demonstration system consists of two software components communicating over a TCP/IP connection using a JavaScript Object Notation (JSON) -based message protocol. The JSON protocol is designed to be extensible, supporting new message types without architectural changes to either the client or host software component. This allows for simple future expansion to various additional physiological data types.
The host software is an embedded application running on the VitalSense hardware. It is responsible for RF signal emission and acquisition via a configurable FPGA pipeline, RF-PMD processing, and algorithm execution. HR and RR measurement results are produced and transmitted to the client software for display and logging.
The client software is an application that provides a graphical user interface (GUI), live HR and RR data plotting, and vital signs data export functionality. The client software connects to the device by specifying the device IP address and TCP port number.
4.3 The VitalSense Cloud
Additionally, the embedded host application on the VitalSense device also offers an IoT cloud interface implementation complying with industry standards. High level cloud communication is achieved using an Application Programming Interface (API) according to an established and easily extensible Interface Control Document (ICD). The VitalSense device application can receive incoming commands, send notifications, and publish data/results to secure cloud services. The device can operate with or without a network (cellular) connection and access to the cloud.
5. PERFORMANCE EVALUATION
5.1 Test Design
Evaluation was conducted across three complementary test phases in November–December 2025, progressing from exploratory characterization to full algorithm integration:
Phase 1 Structured Multi-Subject “Manual Analysis” Study: Five subjects each completed 15 measurements across three physiological states (at rest, elevated post-exercise, and recovery), yielding 75 HR and 75 RR data points. HR reference was a PulseOx device (OxyKnight CF-100); RR reference was manual breath-counting timed by a trained observer. Data were first processed with a hybrid manual–visual analysis approach.
Phase 2 Automated Algorithm Re-Analysis: The same RF dataset was reprocessed with a refined, fully automated first-generation HR/RR algorithm. Performance was re-evaluated against the original reference data.
Phase 3 Proof-of-Concept Demonstration: The algorithm was integrated into production demonstration software. One subject completed 30 HR measurements across all three physiological states to validate end-to-end software performance.
Tolerance criteria were held constant across all phases: HR within ±10% of reference or ±5 bpm (whichever is greater); RR within ±3 brpm.
5.2 Results
The following table summarizes accuracy across all test phases:
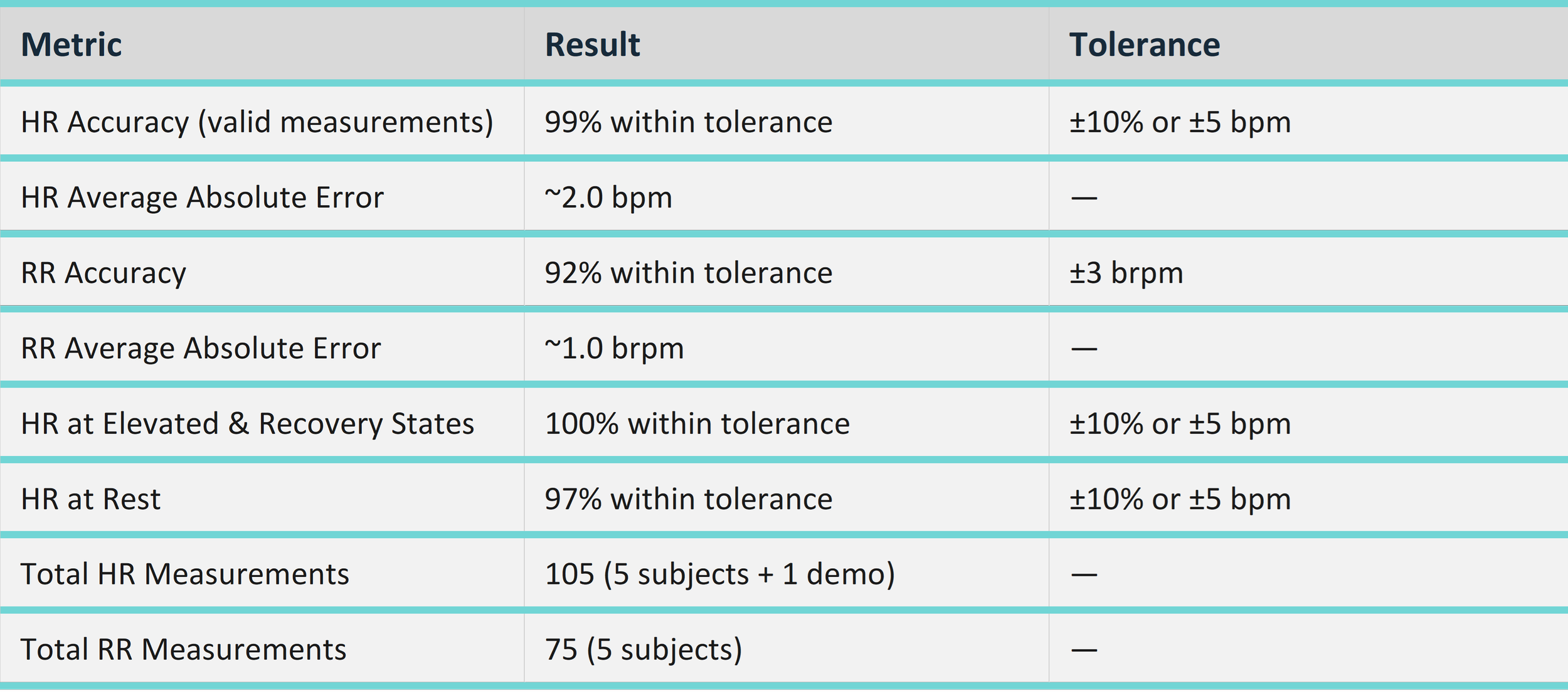
HR accuracy was consistent across physiological states. Elevated and recovery conditions, where cardiac signals are stronger, yielded 100% of valid measurements within tolerance. Resting conditions, where cardiac signal amplitude is lower, still achieved 97% accuracy. Average absolute HR error across all 105 measurements was approximately 2.0 bpm.
RR accuracy was equally consistent: 92% within the ±3 brpm tolerance target across all subjects and all physiological conditions, with an average absolute error of approximately 1.0 brpm. Notably, all 75 RR measurements returned a valid numeric result indicating no algorithm failures or NaN outputs.
Approximately 10% of HR measurements did not return a valid estimate, primarily due to early-measurement subject motion and algorithm search-bound misalignment for outlier physiological states. These limitations are well-characterized, bounded in scope, and addressable through targeted algorithm improvements described below.
6. PATH FORWARD
Building on these results, the following development priorities have been identified to advance the platform toward clinical and commercial readiness:
Expand test population: additional subjects across age, BMI, sex, and morphology ranges to characterize performance boundaries.
Detection range and geometry characterization: systematic testing of range limits, subject orientation variability, and antenna placement optimization.
Motion artifact rejection: implementation and evaluation of data quality gating to reduce invalid-measurement rate from early-measurement motion.
Algorithm search-bound optimization: dynamic configuration of HR estimation bounds to accommodate full target-population HR ranges, including pediatric and athletic populations.
RR signal conditioning: investigation of low-amplitude resting breathing scenarios and SNR optimization for quiet respiratory effort.
Broader clinical and field validation: multi-site studies under IRB oversight to establish performance profiles against FDA-recognized reference standards.
7. CONCLUSION
RF-PMD represents a fundamentally different approach to physiological monitoring, specifically one that exploits the information content already present in ambient RF propagation rather than requiring physical attachment to the subject. The VitalSense platform demonstrates that this approach is not merely theoretically sound but practically achievable at commercially relevant accuracy levels.
The first-generation VitalSense algorithm establishes a strong performance baseline, demonstrating that a fully non-contact, RF-based approach is capable of meeting clinically relevant accuracy thresholds without any physical attachment to the user.
PrīmSphera and the University of Notre Dame are actively pursuing the next development phase to close remaining gaps and advance toward clinical validation.
AUTHORS
Brabec, K.¹, Pratt, T.², Kossler, R.², Adams, C*.¹, & Rauh, C.¹
¹ PrīmSphera, Inc. ² University of Notre Dame
* Corresponding author